One of the things we often have to weigh up, as health professionals, is the balance between risk and benefit.
For example, IF we make a decision towards planning an early birth, there are decisions that involve weighing risks and benefits of doing that. These include, the potential risk of stillbirth if the pregnancy continues, and if labour is induced, the risk of intervention such as forceps and epidural and informing parents that the baby born before 39 weeks is at slightly increased risk of developmental delays that could affect school performance. Because we are talking in terms of risks rather than certainties it is always challenging to have discussions such as these. They are made even more challenging because sometimes, with the benefit of hindsight, it can be seen that a less harmful decision could have been made at the time.
Maternity care providers have risk versus benefit conversations during pregnancy ALL the time. Information that is shared can be consciously or unconsciously affected by their own biases and fears. One such fear prevailing at present is the fear of Covid. I have to tell you that fear of Covid in Western Australia is palpable, AND in my view the response is very much out of proportion to the level of risk. I have heard phrases like “DEFCON 1” and “Ebola like management ” so I know I am not the only person who thinks we are going to extreme and quite unnecessary lengths to “keep safe.”
“Safety “ is a euphemism for death so lets have a look at recent stats concerning the “risk of dying” from Covid in Australia according to age, sex and vaccination status.
For example, IF we make a decision towards planning an early birth, there are decisions that involve weighing risks and benefits of doing that. These include, the potential risk of stillbirth if the pregnancy continues, and if labour is induced, the risk of intervention such as forceps and epidural and informing parents that the baby born before 39 weeks is at slightly increased risk of developmental delays that could affect school performance. Because we are talking in terms of risks rather than certainties it is always challenging to have discussions such as these. They are made even more challenging because sometimes, with the benefit of hindsight, it can be seen that a less harmful decision could have been made at the time.
Maternity care providers have risk versus benefit conversations during pregnancy ALL the time. Information that is shared can be consciously or unconsciously affected by their own biases and fears. One such fear prevailing at present is the fear of Covid. I have to tell you that fear of Covid in Western Australia is palpable, AND in my view the response is very much out of proportion to the level of risk. I have heard phrases like “DEFCON 1” and “Ebola like management ” so I know I am not the only person who thinks we are going to extreme and quite unnecessary lengths to “keep safe.”
“Safety “ is a euphemism for death so lets have a look at recent stats concerning the “risk of dying” from Covid in Australia according to age, sex and vaccination status.
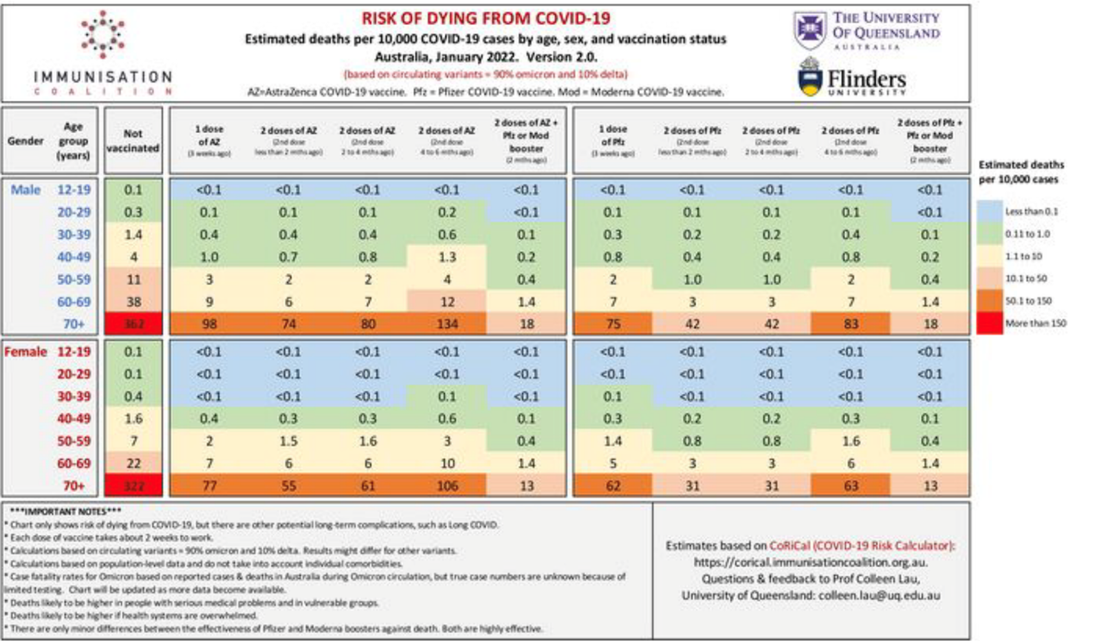
Its pretty obvious from this Australian research that even if you are not vaccinated at all that your risk of dying from Covid is incredibly low especially if you are under the age of 70. For example, if you are an unvaccinated male between the ages of 50 and 59 your risk of dying is only 11 per 10,000 cases and once triple vaxed this drops to 4 in 100,000.
You can also see from this chart that if you are an Australian woman of childbearing age that the risk of dying from Covid is less than 1 per 100,000 especially if you have had any kind of vaccination.
Shouldn’t we be careful ? I hear you ask. I agree we should be careful and I ABSOLUTELY agree that we should be doing all we can to protect our elderly AND 1 in 100,000 young people dying is one too many BUT here is my point.
“how much harm are we prepared to cause to prevent that one death?”
Current approaches to managing Covid in maternity settings is doing WAY more harm than good, in my view. To borrow from another campaign “Covid is a word not a sentence”.
While there are physical harms being caused that I have talked about before on this blog I am also becoming more and more concerned about the long term emotional and psychological scarring we are undoubtably causing. I think that it won’t be too long at all before we look back in horror at our treatment of birthing families during Covid and ask “what were they thinking?”
Pregnancy and Birth is a special time and the experience can’t be regained or memories changed. Anxiety during pregnancy is common and Birth trauma is real, even when everything is apparently fine. Parent / Child bonding can be fragile and the negative, long term sequalae of disordered attachment is well known. What happens during pregnancy and birth is remembered and reflected upon for the rest of that persons’ life ask any 80-year-old mother!! There is much to be concerned about for pregnancy and birth during covid including:
It may be, that even now, some people will look at this very limited list and say “surely that isn’t happening!” It seems draconian, heartless and cruel doesn’t it? While I think stopping people at the door of a nursing home and perhaps even a general hospital where there are sick children or adults is probably necessary, I take you back to my original point, care providers are sworn to “first do no harm” and as far as I can see we are doing tremendous harm to our birthing families for very little benefit.
So, can someone with a brain and a heart STOP this insane approach before we do any more immeasurable harm…. PLEASE!
You can also see from this chart that if you are an Australian woman of childbearing age that the risk of dying from Covid is less than 1 per 100,000 especially if you have had any kind of vaccination.
Shouldn’t we be careful ? I hear you ask. I agree we should be careful and I ABSOLUTELY agree that we should be doing all we can to protect our elderly AND 1 in 100,000 young people dying is one too many BUT here is my point.
“how much harm are we prepared to cause to prevent that one death?”
Current approaches to managing Covid in maternity settings is doing WAY more harm than good, in my view. To borrow from another campaign “Covid is a word not a sentence”.
While there are physical harms being caused that I have talked about before on this blog I am also becoming more and more concerned about the long term emotional and psychological scarring we are undoubtably causing. I think that it won’t be too long at all before we look back in horror at our treatment of birthing families during Covid and ask “what were they thinking?”
Pregnancy and Birth is a special time and the experience can’t be regained or memories changed. Anxiety during pregnancy is common and Birth trauma is real, even when everything is apparently fine. Parent / Child bonding can be fragile and the negative, long term sequalae of disordered attachment is well known. What happens during pregnancy and birth is remembered and reflected upon for the rest of that persons’ life ask any 80-year-old mother!! There is much to be concerned about for pregnancy and birth during covid including:
- Fathers not being allowed to enter a maternity hospital or if they are allowed in, there are MANY barriers including mask and vaccination mandates, and time limits
- Fathers seeing ultrasound in a hospital car park via facetime
- Requirement for support people to wear full PPE during those very first precious moments when greeting the new baby and establishing attunement which necessarily involves the parent and baby’s WHOLE face.
- Siblings being denied entry
- Extended family members being denied entry
- No support person allowed in antenatal clinic. There are many situations that can arise in pregnancy when bad news might need to be broken and immediate comfort and support needed. NOT TO MENTION having another pair of ears in the room when explanations are given and another person to ask questions not thought of by the other person.
- Time limits for support during birth
It may be, that even now, some people will look at this very limited list and say “surely that isn’t happening!” It seems draconian, heartless and cruel doesn’t it? While I think stopping people at the door of a nursing home and perhaps even a general hospital where there are sick children or adults is probably necessary, I take you back to my original point, care providers are sworn to “first do no harm” and as far as I can see we are doing tremendous harm to our birthing families for very little benefit.
So, can someone with a brain and a heart STOP this insane approach before we do any more immeasurable harm…. PLEASE!
 RSS Feed
RSS Feed
