I was intrigued and disappointed when I was alerted to this recently published paper by Hiscock et al
Intrigued because the authors had taken an interesting novel approach to exploring the potential connection between gestation at birth and later school performance. Disappointed because they only looked at the potential impact of being born at 39 weeks vs 40-41 weeks on later school performance thereby missing a good opportunity to confirm …or refute… the narrative of 39 being the line in the sand for induction of labour at ‘term’ rather than 38 weeks.
There have now been a number of observational cohort studies that have reported that if you are born preterm or very preterm you are more likely to struggle at school. The reasons for this are numerous and all completely physiological and logical. The studies that concern me however, are the ones that have indicated that later cognitive function (school performance) is worse for those babies born ‘early term’ i.e., 37-39 weeks.
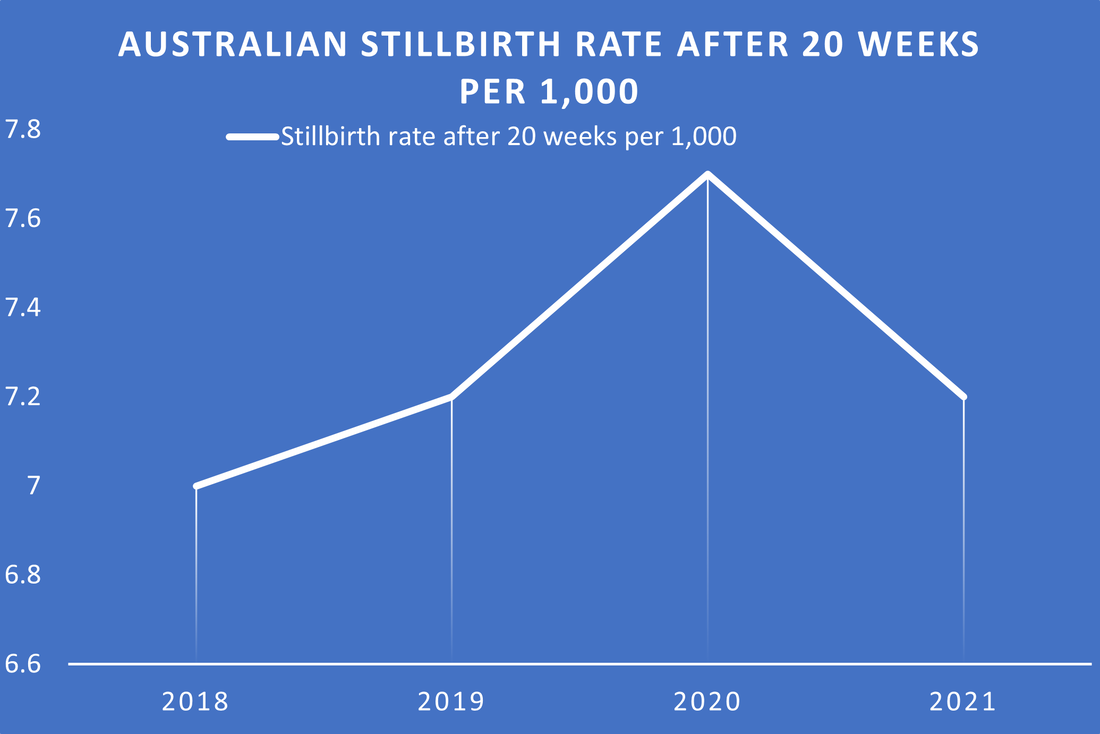
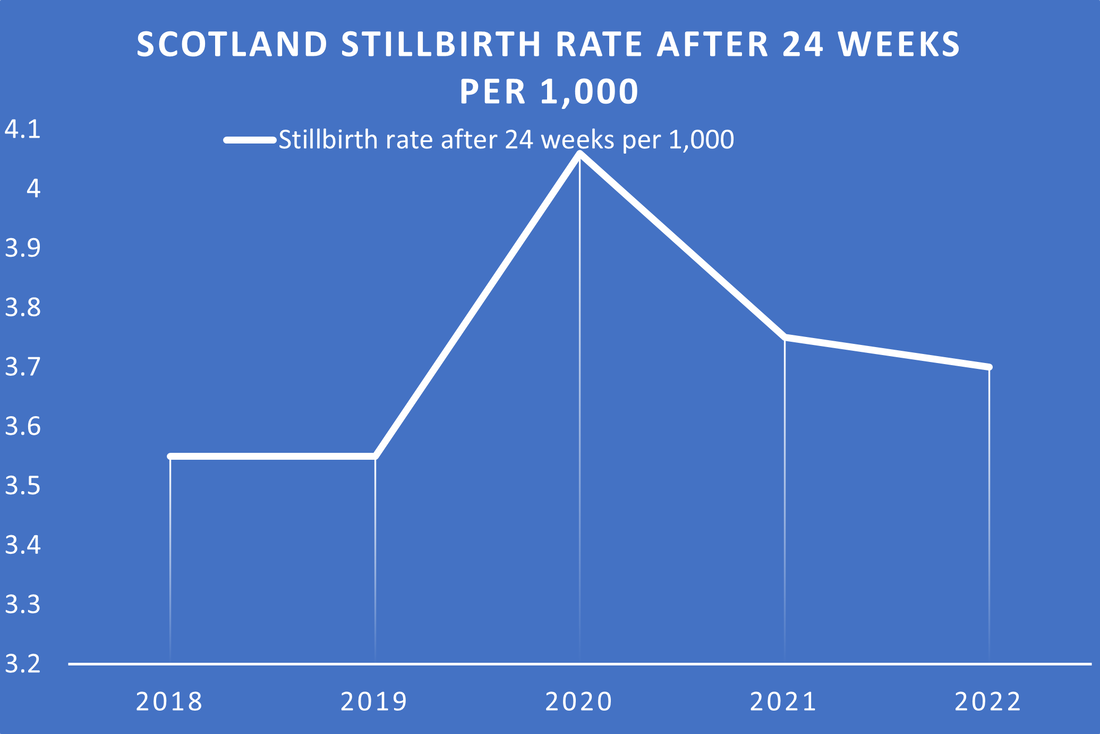
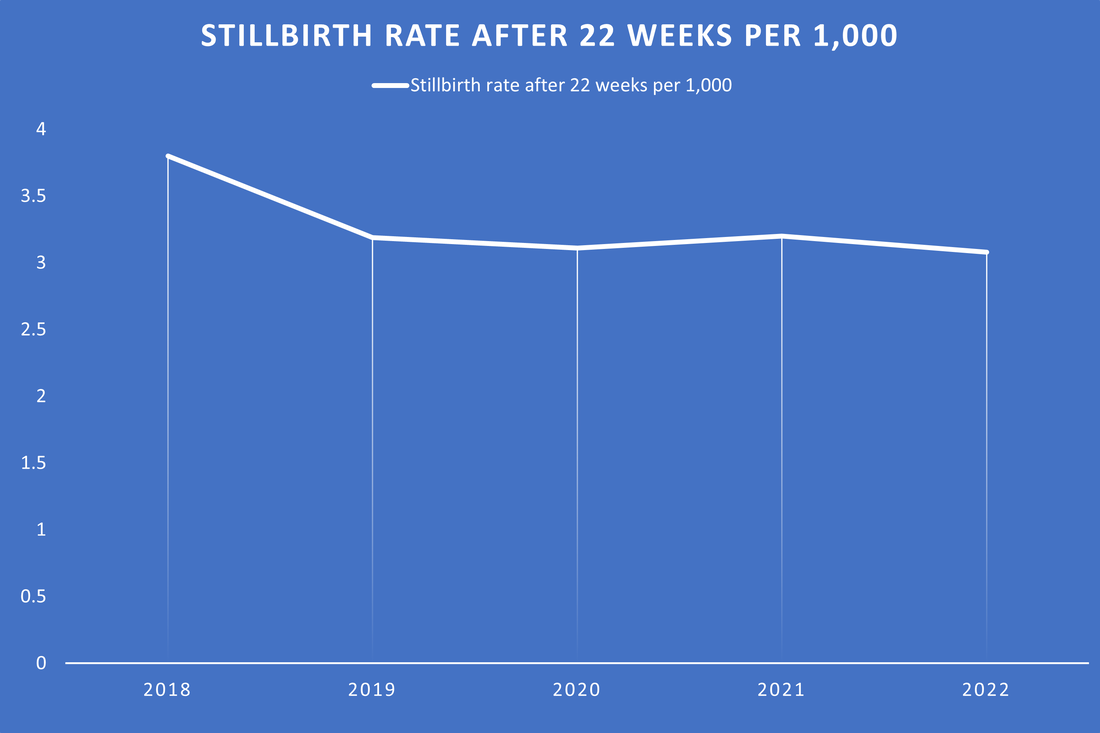
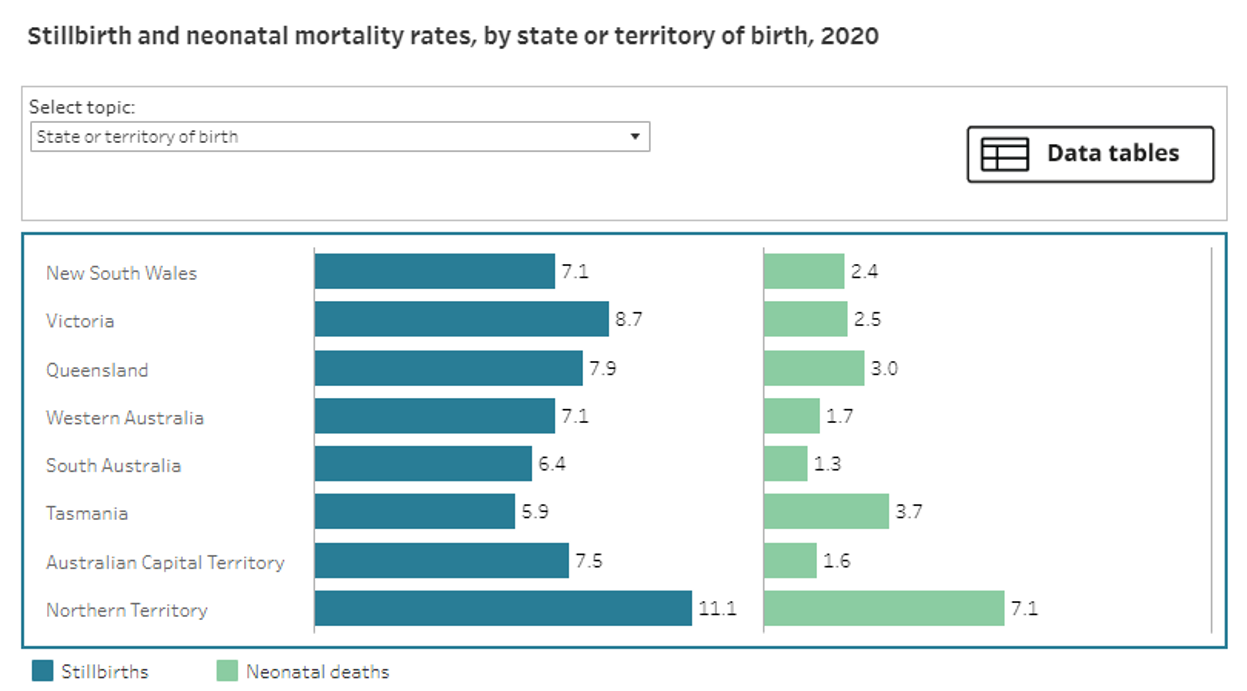
These studies concern me because if you draw a line in the sand at 39 weeks you will inevitably increase risk of stillbirth at 38 weeks. Now, those who would argue that you will prevent all term stillbirth if you deliver everyone at 37 weeks, miss the point that the risk of stillbirth isn’t the same for all ‘early term’ fetuses’. This is because if you look at the fetus at risk (FAR) of stillbirth in pretty much any set of perinatal data collected anywhere in the world you see this kind of graph (AIHW data 2021)
Intrigued because the authors had taken an interesting novel approach to exploring the potential connection between gestation at birth and later school performance. Disappointed because they only looked at the potential impact of being born at 39 weeks vs 40-41 weeks on later school performance thereby missing a good opportunity to confirm …or refute… the narrative of 39 being the line in the sand for induction of labour at ‘term’ rather than 38 weeks.
There have now been a number of observational cohort studies that have reported that if you are born preterm or very preterm you are more likely to struggle at school. The reasons for this are numerous and all completely physiological and logical. The studies that concern me however, are the ones that have indicated that later cognitive function (school performance) is worse for those babies born ‘early term’ i.e., 37-39 weeks.
These studies concern me because if you draw a line in the sand at 39 weeks you will inevitably increase risk of stillbirth at 38 weeks. Now, those who would argue that you will prevent all term stillbirth if you deliver everyone at 37 weeks, miss the point that the risk of stillbirth isn’t the same for all ‘early term’ fetuses’. This is because if you look at the fetus at risk (FAR) of stillbirth in pretty much any set of perinatal data collected anywhere in the world you see this kind of graph (AIHW data 2021)
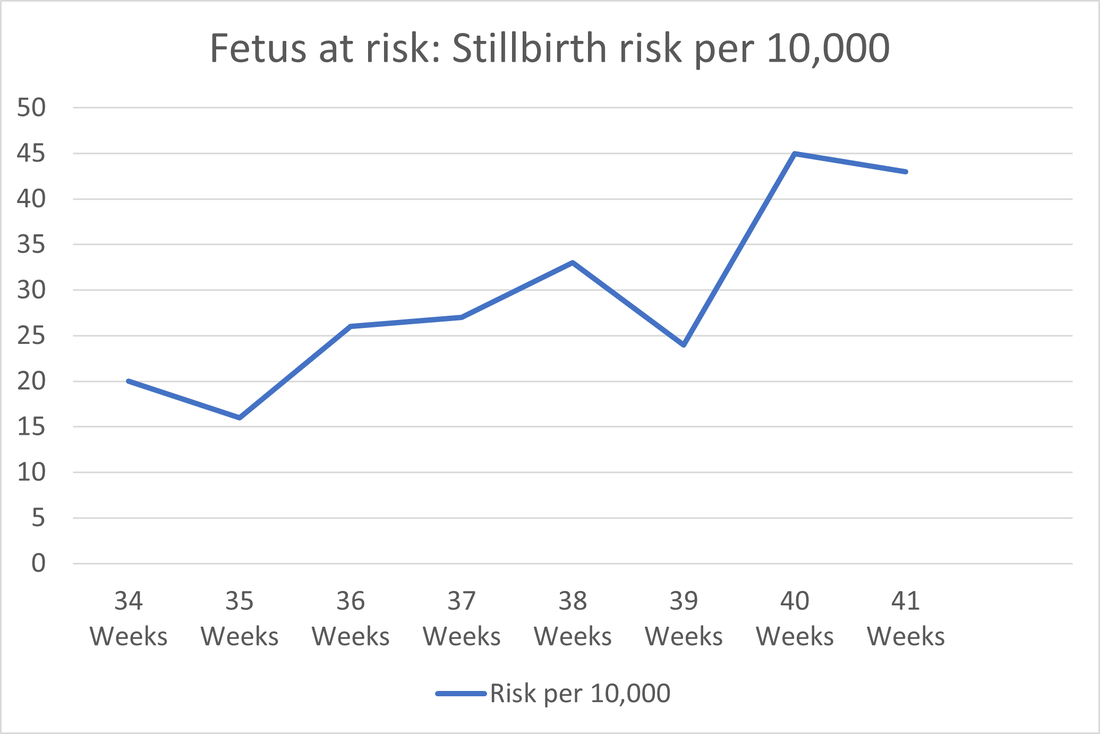
The thing to notice here is that there is always a ‘hump’ in stillbirth risk /rate at 38 weeks. This means that if you have a policy or , as in the USA, a mandate that 39 weeks is the magic gestation to induce labour at rather than 38 weeks which some now call ‘early term,’ then inevitably some babies won’t make it that extra week and they will end up stillborn.
To go back to the Hiscock et al paper the authors recognise there has been some controversy about inducing birth before 40 weeks hence the reason for their study to show that you apparently do no harm to later cognitive function at school if you induce labour at 39 weeks.
The shame is I actually don’t think there is much argument that 39 weeks is not okay, in fact the issue that proponents of the ‘wait til 39 week’ have is that inducing the baby before 39 weeks is bad. The current narrative is that you do harm by stunting brain growth and therefore later school performance if you deliver a baby before 39 weeks.
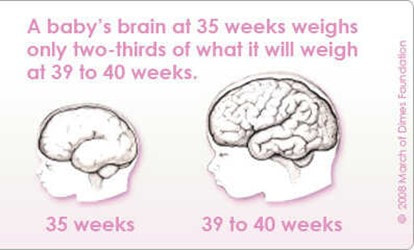
Just in case you are not up with that narrative, its based on the idea that if a baby is born before 39 weeks that the brain is forever stunted, as apparently (according to some, see pic) the brain doesn’t grow and develop outside the uterus so the child born preterm is stuck with a small brain for the rest of their life!
To go back to the Hiscock et al paper the authors recognise there has been some controversy about inducing birth before 40 weeks hence the reason for their study to show that you apparently do no harm to later cognitive function at school if you induce labour at 39 weeks.
The shame is I actually don’t think there is much argument that 39 weeks is not okay, in fact the issue that proponents of the ‘wait til 39 week’ have is that inducing the baby before 39 weeks is bad. The current narrative is that you do harm by stunting brain growth and therefore later school performance if you deliver a baby before 39 weeks.
Just in case you are not up with that narrative, its based on the idea that if a baby is born before 39 weeks that the brain is forever stunted, as apparently (according to some, see pic) the brain doesn’t grow and develop outside the uterus so the child born preterm is stuck with a small brain for the rest of their life!
I am really not sure why this is even a thing, as it defies logic. Why would every other part of the preterm baby still grow after birth except the baby’s brain? It also is an argument that doesn’t make sense physiologically. The human fetus’ skull is disproportionately large so the brain grows as large as possible before the baby’s skull has to safely traverse the human pelvis without killing the mother! Further, the baby’s skull has sutures to fuse, and fontanelles to close precisely to allow for extrauterine brain growth. In sum, the human gestational length is limited by how big the baby’s head can get and it means the human baby is born helpless but with as big a brain as possible to fit into its disproportionately large skull at birth. Of course the brain develops and grows after birth to say that it doesn’t is nonsense, I challenge anyone wandering through a room of 8 year old school kids to tell their gestation at birth based on hat size! Ridiculous right?
Further, IMHO, the studies that are relied upon to show that children born before 39 weeks might struggle at school are mainly reliant on one primary outcome (performance at school) or IQ test or similar and are so confounded with other variables also associated with reasons for IOL and cognitive development in the years between birth and school as to be rubbish. Unfortunately, not everyone thinks they are rubbish and so they are being used to make a case for waiting until 39 weeks to induce labour.
Just looking at a couple of these:
Bentley et al paper, a cohort study, incidentally the one that really seems to be responsible for the “wait until 39 week” narrative in Australia. The problem with this and others like it is the reason for the preterm birth wasn’t taken into consideration. This is a really important confounder as other studies I have summarised below indicate. The other thing about this study is that they reported association between early planned birth and elevated risk of poor development at school age. Claiming that the timing of birth is modifiable so more “strategies to inform more judicious decision-making are needed to ensure optimal child health and development” Two things to note, the risk of ‘developmentally high risk’ at 38 weeks is reported to be aRR 1.06 (1.01–1.10), when you consider a 95% CI which includes 1.00 is statistically insignificant the fact that it ranges from 1.01 means that this is the smallest teeniest, tiniest increased risk you can get ! Therefore, basing practice change on this study and advising planned birth at 39 weeks is hardly compelling especially given findings from other studies that also point out that adjusting for the reason for IOL is kinda important e.g.:
Gleason et al conducted a large secondary analysis of spontaneous onset births from data collected for the US Collaborative Perinatal Project (1959–76) and reported that “40–41 weeks may be the ideal delivery window for optimal neurodevelopmental outcomes” Interestingly they not only did not report the reason for the preterm / early term birth they actually excluded those with gestational hypertension, pre-eclampsia or gestational diabetes, as in their words these conditions may “influence placental sufficiency and subsequent neurocognitive outcomes.”!! Interestingly they excluded or adjusted for potential confounders present during the pregnancy but not the reason for the IOL nor for anything that may…or may not have occurred during the 8 years of subsequent childhood. And they stated in their limitations “the results may be confounded by not adjusting for the indication for induction, which may influence developmental outcomes.” May… MAY ??!!
The reason for early birth is just one important confounder, here are many more important confounders such as educational attainment of the parents! e.g.:
Quigley et al conducted a cohort study of seven thousand six hundred and fifty children born in 2000–2001 and attending school in England in 2006. They reported late preterm and early term birth are associated with an increased risk of poorer educational achievement at age 5 years. But then they say birth before full term has a smaller effect than the child's sex and age within the school year, and their mother's level of education, they reported that gestation was “one more element that affects the risk profile of the child”. They gave a good example of what they meant: the percentage of children who had not reached a good level of achievement was 38% in children whose mothers had a university degree, 55% in children whose mothers had other qualifications and 76% in children whose mother had no qualifications. The additional impact of late preterm birth (ie, RR=1.12) would increase these risks to 42%, 62% and 85%, respectively.
Quigley’s study is a really good example that shows that looking at just one factor which is also associated with school performance can massively impact results especially if its more highly associated with school performance than gestation at birth itself. It shows pretty well that there really are too many confounders that may be impacting on school performance and that gestation at birth may be one really minor one of dozens if not hundreds more.
Also, in most of these studies confounders present during the pregnancy may have been included in adjusting the analysis BUT ‘nurture’ between birth and the age of assessment of school performance wasn’t. So things like BOTH parents education, parental IQ, any changes in socio economic status between birth and school, number of hospital visits in childhood related to the reason for the prematurity/gestation at birth etc etc should ALL have been used. That they were not used is an indicator about just how difficult adjusting for confounders for this kind of study is, but also shows the potential danger of relying on results from these, very good but, observational cohort studies upon which to base practice.
I guess what I am trying to say is that since earlier studies reporting a potential link between gestation at birth and school performance there is a growing weight of evidence that 39 weeks isn’t as magic a gestation as might have been first thought. That perhaps, given the risk of stillbirth is highest at 38 weeks and that this is really ‘term’ AND if the baby is dead then school performance isn’t something the parents need to worry about, perhaps we need to rethink 39 weeks and move the line in the sand to 38 instead?
Further, that even if you happen to believe that birth before 39 weeks alters cognitive function surely it is not too long a bow to draw to also consider that parenting along with a host of other confounders, I’ve already mentioned, has a massive influence on how the child does at school and if the child really needs to be born at 38 weeks then there is ample time and many things parents can do to overcome any potential deficit by stimulating their child’s cognitive development…one of the most fun and rewarding things about parenting IMHO!
So to return to my disappointment about this new study. It showed very nicely that being born at 39 weeks doesn’t impact on school performance when compared to being born at 40-41 weeks. It is a real shame they didn’t also look at birth at 38 weeks as if there was a similar lack of impact.. which I suspect is probably the case, then we could all heave a sigh of relief and safely move the 39 weeks rule/narrative to 38 weeks and in the process probably save some babies lives at no expense to school performance!
References:
Bentley JP, Roberts CL, Bowen JR, Martin AJ, Morris JM, Nassar N. Planned birth before 39 weeks and child development: a population-based study. Pediatrics. 2016;138(6):1-9. doi:10.1542/peds.2016-2002
Gleason JL, Gilman SE, Sundaram R, et al. Gestational age at term delivery and children’s neurocognitive development. Int J Epidemiol. 2022;50(6):1814-1823. doi:10.1093/ije/dyab134
MacKay DF, Smith GCS, Dobbie R, Pell JP. Gestational age at delivery and special educational need: retrospective cohort study of 407,503 schoolchildren. PLoS Med. 2010;7(6):e1000289. doi:10.1371/journal.pmed.1000289
Selvaratnam RJ, Wallace EM, Rolnik DL, et al. Elective induction of labour at full-term gestations and childhood school outcomes. J Paediatr Child Health. 2023;59(9):1028-1034. doi:10.1111/jpc.16449
Further, IMHO, the studies that are relied upon to show that children born before 39 weeks might struggle at school are mainly reliant on one primary outcome (performance at school) or IQ test or similar and are so confounded with other variables also associated with reasons for IOL and cognitive development in the years between birth and school as to be rubbish. Unfortunately, not everyone thinks they are rubbish and so they are being used to make a case for waiting until 39 weeks to induce labour.
Just looking at a couple of these:
Bentley et al paper, a cohort study, incidentally the one that really seems to be responsible for the “wait until 39 week” narrative in Australia. The problem with this and others like it is the reason for the preterm birth wasn’t taken into consideration. This is a really important confounder as other studies I have summarised below indicate. The other thing about this study is that they reported association between early planned birth and elevated risk of poor development at school age. Claiming that the timing of birth is modifiable so more “strategies to inform more judicious decision-making are needed to ensure optimal child health and development” Two things to note, the risk of ‘developmentally high risk’ at 38 weeks is reported to be aRR 1.06 (1.01–1.10), when you consider a 95% CI which includes 1.00 is statistically insignificant the fact that it ranges from 1.01 means that this is the smallest teeniest, tiniest increased risk you can get ! Therefore, basing practice change on this study and advising planned birth at 39 weeks is hardly compelling especially given findings from other studies that also point out that adjusting for the reason for IOL is kinda important e.g.:
Gleason et al conducted a large secondary analysis of spontaneous onset births from data collected for the US Collaborative Perinatal Project (1959–76) and reported that “40–41 weeks may be the ideal delivery window for optimal neurodevelopmental outcomes” Interestingly they not only did not report the reason for the preterm / early term birth they actually excluded those with gestational hypertension, pre-eclampsia or gestational diabetes, as in their words these conditions may “influence placental sufficiency and subsequent neurocognitive outcomes.”!! Interestingly they excluded or adjusted for potential confounders present during the pregnancy but not the reason for the IOL nor for anything that may…or may not have occurred during the 8 years of subsequent childhood. And they stated in their limitations “the results may be confounded by not adjusting for the indication for induction, which may influence developmental outcomes.” May… MAY ??!!
The reason for early birth is just one important confounder, here are many more important confounders such as educational attainment of the parents! e.g.:
Quigley et al conducted a cohort study of seven thousand six hundred and fifty children born in 2000–2001 and attending school in England in 2006. They reported late preterm and early term birth are associated with an increased risk of poorer educational achievement at age 5 years. But then they say birth before full term has a smaller effect than the child's sex and age within the school year, and their mother's level of education, they reported that gestation was “one more element that affects the risk profile of the child”. They gave a good example of what they meant: the percentage of children who had not reached a good level of achievement was 38% in children whose mothers had a university degree, 55% in children whose mothers had other qualifications and 76% in children whose mother had no qualifications. The additional impact of late preterm birth (ie, RR=1.12) would increase these risks to 42%, 62% and 85%, respectively.
Quigley’s study is a really good example that shows that looking at just one factor which is also associated with school performance can massively impact results especially if its more highly associated with school performance than gestation at birth itself. It shows pretty well that there really are too many confounders that may be impacting on school performance and that gestation at birth may be one really minor one of dozens if not hundreds more.
Also, in most of these studies confounders present during the pregnancy may have been included in adjusting the analysis BUT ‘nurture’ between birth and the age of assessment of school performance wasn’t. So things like BOTH parents education, parental IQ, any changes in socio economic status between birth and school, number of hospital visits in childhood related to the reason for the prematurity/gestation at birth etc etc should ALL have been used. That they were not used is an indicator about just how difficult adjusting for confounders for this kind of study is, but also shows the potential danger of relying on results from these, very good but, observational cohort studies upon which to base practice.
I guess what I am trying to say is that since earlier studies reporting a potential link between gestation at birth and school performance there is a growing weight of evidence that 39 weeks isn’t as magic a gestation as might have been first thought. That perhaps, given the risk of stillbirth is highest at 38 weeks and that this is really ‘term’ AND if the baby is dead then school performance isn’t something the parents need to worry about, perhaps we need to rethink 39 weeks and move the line in the sand to 38 instead?
Further, that even if you happen to believe that birth before 39 weeks alters cognitive function surely it is not too long a bow to draw to also consider that parenting along with a host of other confounders, I’ve already mentioned, has a massive influence on how the child does at school and if the child really needs to be born at 38 weeks then there is ample time and many things parents can do to overcome any potential deficit by stimulating their child’s cognitive development…one of the most fun and rewarding things about parenting IMHO!
So to return to my disappointment about this new study. It showed very nicely that being born at 39 weeks doesn’t impact on school performance when compared to being born at 40-41 weeks. It is a real shame they didn’t also look at birth at 38 weeks as if there was a similar lack of impact.. which I suspect is probably the case, then we could all heave a sigh of relief and safely move the 39 weeks rule/narrative to 38 weeks and in the process probably save some babies lives at no expense to school performance!
References:
Bentley JP, Roberts CL, Bowen JR, Martin AJ, Morris JM, Nassar N. Planned birth before 39 weeks and child development: a population-based study. Pediatrics. 2016;138(6):1-9. doi:10.1542/peds.2016-2002
Gleason JL, Gilman SE, Sundaram R, et al. Gestational age at term delivery and children’s neurocognitive development. Int J Epidemiol. 2022;50(6):1814-1823. doi:10.1093/ije/dyab134
MacKay DF, Smith GCS, Dobbie R, Pell JP. Gestational age at delivery and special educational need: retrospective cohort study of 407,503 schoolchildren. PLoS Med. 2010;7(6):e1000289. doi:10.1371/journal.pmed.1000289
Selvaratnam RJ, Wallace EM, Rolnik DL, et al. Elective induction of labour at full-term gestations and childhood school outcomes. J Paediatr Child Health. 2023;59(9):1028-1034. doi:10.1111/jpc.16449
 RSS Feed
RSS Feed
