I recently presented on this title at the Australian College of Midwives conference in Adelaide. Several of my colleagues asked me afterwards if I could point them to a paper or website about the Australian data I included in my presentation.
I said that everything I presented was publicly available but I did promised them that I would publish this on my Blog and so here it is…all in one spot!
The title of my presentation was “what were we thinking?” and what I asked them to ponder was this…
Shortly after the Covid pandemic was declared and lock down restrictions announced the Royal Australian and New Zealand College announced the following guidance for antenatal care provision:
Here is a figure showing what happened to antenatal service provision in Australia in 2020:
I said that everything I presented was publicly available but I did promised them that I would publish this on my Blog and so here it is…all in one spot!
The title of my presentation was “what were we thinking?” and what I asked them to ponder was this…
Shortly after the Covid pandemic was declared and lock down restrictions announced the Royal Australian and New Zealand College announced the following guidance for antenatal care provision:
- Reducing, postponing and/or increasing the interval between antenatal visits
- Limiting time of all antenatal visits to less than 15 minutes
- Using telehealth consultations as a replacement, or in addition to, routine visits
- Cancelling face to face antenatal classes
- Limiting visitors (partner only) while in hospital
- Considering early discharge from hospital
- Minimise risk of neonatal complications by avoiding early planned birth unless clearly clinically indicated
Here is a figure showing what happened to antenatal service provision in Australia in 2020:
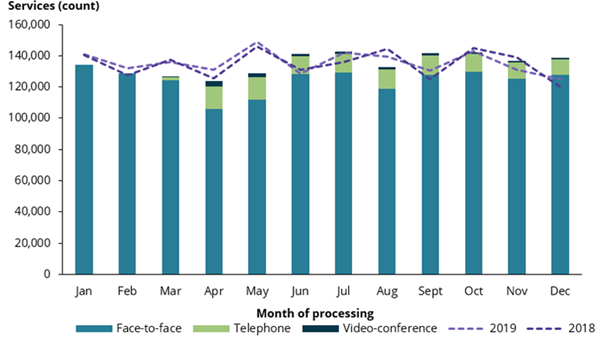
We can see that antenatal service provision dropped through most months of 2020 when compared to 2018 and 2019 (the dotted lines). The commentary that goes with this figure suggests that the drop in face-to-face service was “largely offset” by the advent of telehealth which was added to the MBS to cover antenatal care on 13 March 2020, (DoH 2020b). Other interesting things about this figure to note:
The answer …I’m afraid is... “you can’t”.
Now, unfortunately, we have the evidence of the impact of reducing face to face visits and substituting them with a phone conversation and….it isn’t good ☹:
We can see that antenatal service provision dropped through most months of 2020 when compared to 2018 and 2019 (the dotted lines). The commentary that goes with this figure suggests that the drop in face-to-face service was “largely offset” by the advent of telehealth which was added to the MBS to cover antenatal care on 13 March 2020, (DoH 2020b). Other interesting things about this figure to note:
- During the period March to December 2020, telehealth services were most common in Victoria, comprising nearly 15% of antenatal care services processed during this period.
- Across the country, telephone consults were more common than video-conference, comprising 87.5% of antenatal telehealth services.
The answer …I’m afraid is... “you can’t”.
Now, unfortunately, we have the evidence of the impact of reducing face to face visits and substituting them with a phone conversation and….it isn’t good ☹:
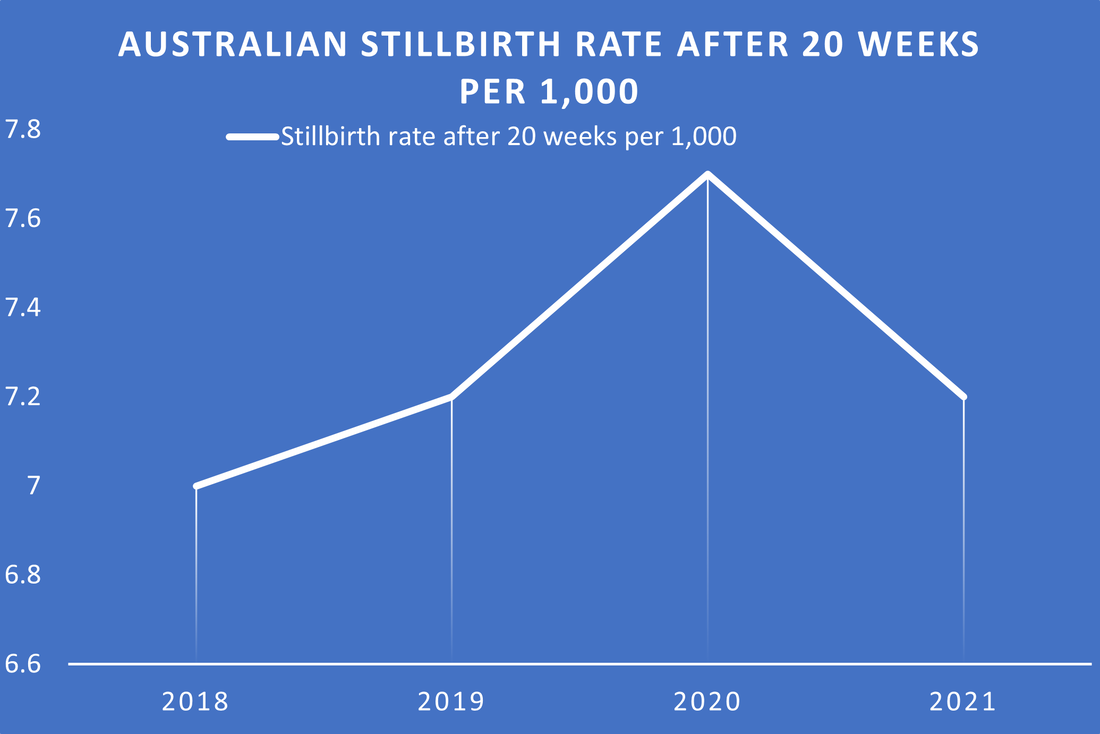
This is AIHW data showing that the stillbirth rate in Australia in 2020 went up .5 per thousand and minimum data from 2021 indicate that the rate may have returned roughly to pre-covid levels). “point 5 per thousand doesn’t sound like much” I hear you say but the actual number that .5 per thousand represents is more than 100 babies. Let me say that again, there were 100 more stillbirths in Australia in 2020 than in 2019…or 2018 for that matter. Did the purposeful reduction of antenatal service provision result in an increase in Stillbirth?
My answer is YES and here is why I think so.
Firstly, I want to point you to Scotland perinatal data. I don’t think there is much doubt that Scotland collect and publish the best perinatal data collection in the world. They collect and publish their data monthly and while there is a little bit of inaccuracy when you publish any kind of morbidity /mortality data that quickly it is mainly accurate especially for 2020 .
My answer is YES and here is why I think so.
Firstly, I want to point you to Scotland perinatal data. I don’t think there is much doubt that Scotland collect and publish the best perinatal data collection in the world. They collect and publish their data monthly and while there is a little bit of inaccuracy when you publish any kind of morbidity /mortality data that quickly it is mainly accurate especially for 2020 .
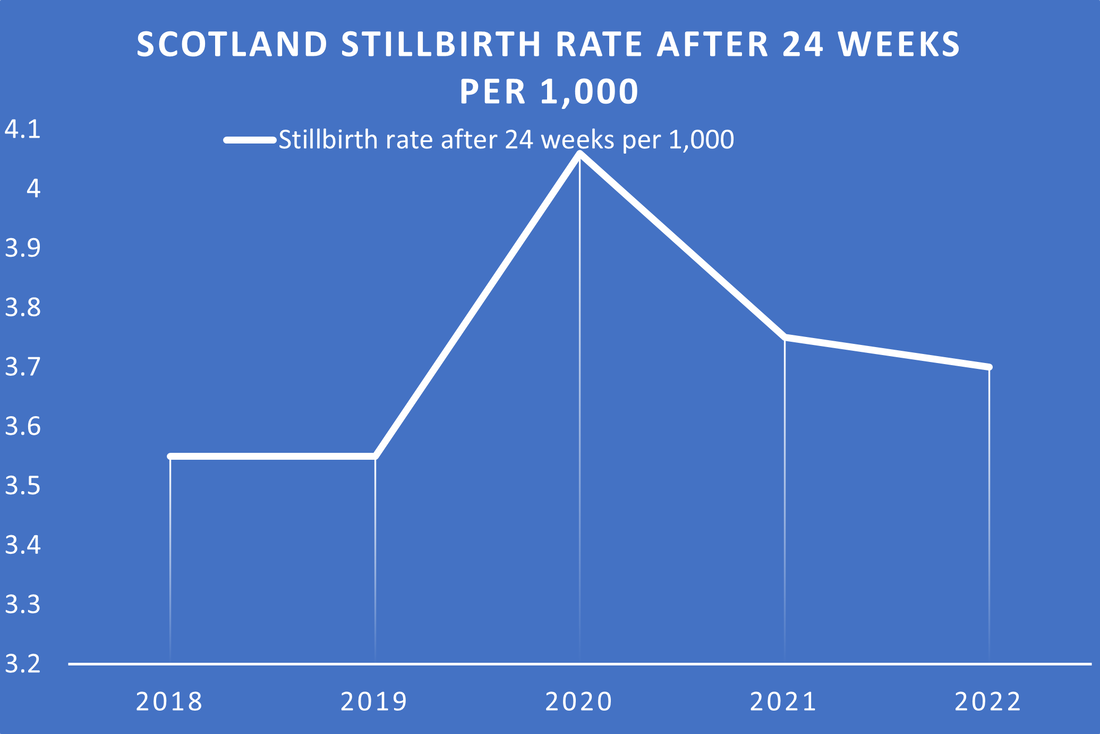
You can see that the figure shows a remarkable similarity to Australia in that the Stillbirth rate in Scotland also increased .5 per thousand in 2020 and by end of 2022 has not quite returned to pre covid levels. Did Scotland have similar disruption to antenatal service provision as Australia? Yes they had lengthy country wide lock downs and just as in Australia, maternity care was altered to have less antenatal visits in order to “protect both staff and mother”
So how do I know that it was disruption in antenatal service provision and not Covid infection itself that caused this awful rise in stillbirth rate in these high income countries?
Well lets have a look at Sweden?
I think it would be fair to say that Sweden’s “let it rip” approach to the Pandemic drew the astonishment of the rest of the world. As far as I can recall they were one, and probably even the only, high income country that took this approach. They kept schools open, asked their population to socially distance, stay at home if they felt unwell and work from home if they could. So looking at Swedish stillbirth rate in 2020 should inform us whether or not it was antenatal service provision interruption or Covid itself that cause the increase in stillbirth rate..right….?
So how do I know that it was disruption in antenatal service provision and not Covid infection itself that caused this awful rise in stillbirth rate in these high income countries?
Well lets have a look at Sweden?
I think it would be fair to say that Sweden’s “let it rip” approach to the Pandemic drew the astonishment of the rest of the world. As far as I can recall they were one, and probably even the only, high income country that took this approach. They kept schools open, asked their population to socially distance, stay at home if they felt unwell and work from home if they could. So looking at Swedish stillbirth rate in 2020 should inform us whether or not it was antenatal service provision interruption or Covid itself that cause the increase in stillbirth rate..right….?
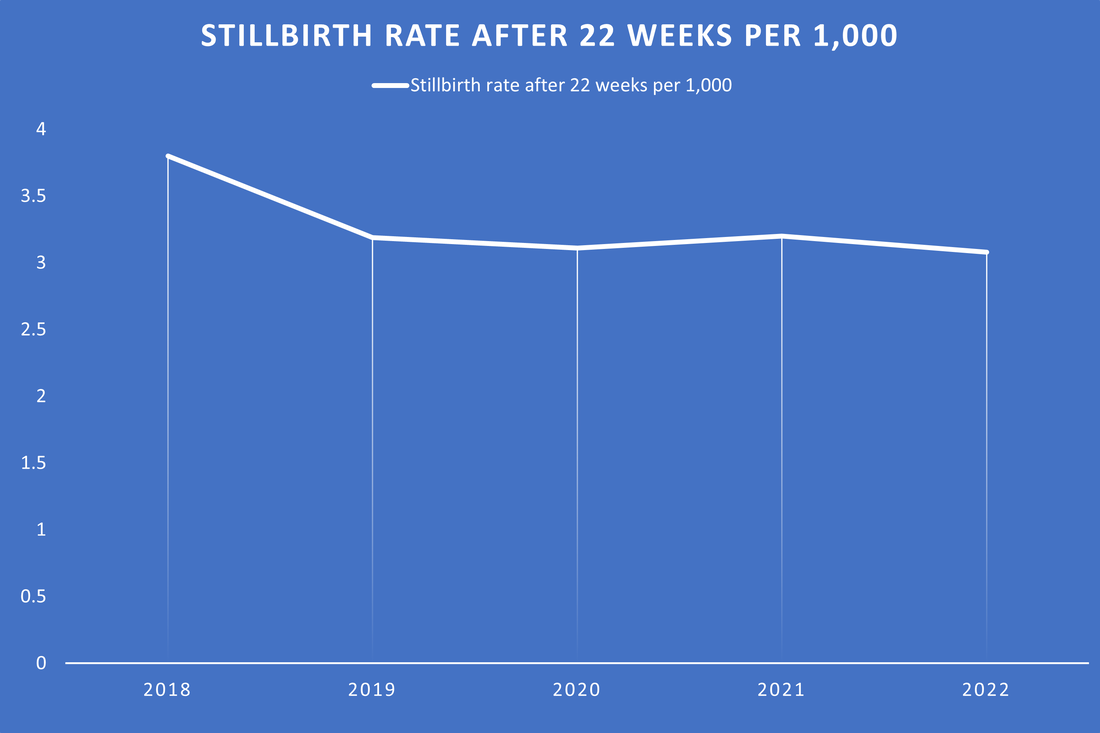
Well as Sweden had WAY more Covid in the community than Australia did in 2020 but maintained a static stillbirth rate it looks like it was the antenatal service disruption that caused an increase in stillbirth!!
By the way the maternal death rate in Sweden in 2020 was 5 per 100,000 a rate that has been static for many years before and since. So no… the static stillbirth rate did not come at the cost of mothers lives.
Still don’t quite believe me?
Lets look at Victoria. As any Melbournian would tell you they had the strictest, longest lockdown in the world.
AIHW data tell us that they had the largest uptake of telehealth (by telephone) in Australia. 15% of their reduced visits were by telephone.
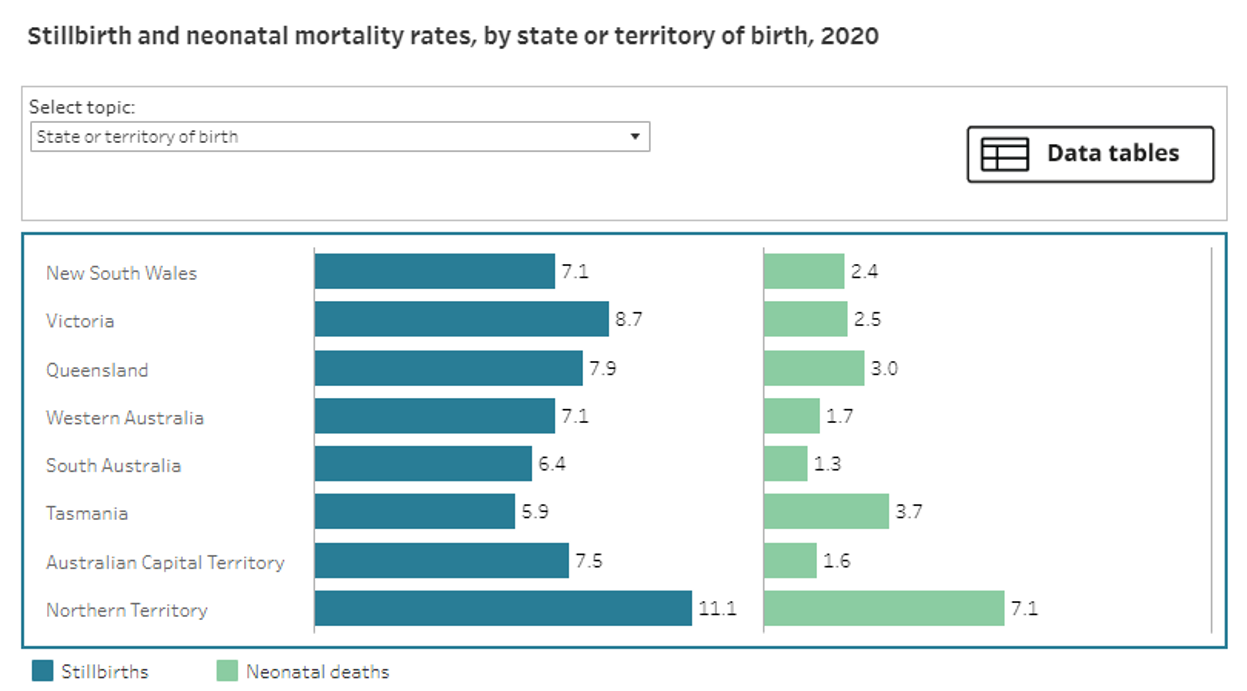
The AIHW figure below shows Victoria had far and away the worse stillbirth rate in Australia in 2020 rising from 6 per thousand in 2017-2019 to 8.7 per thousand in 2020.
By the way the maternal death rate in Sweden in 2020 was 5 per 100,000 a rate that has been static for many years before and since. So no… the static stillbirth rate did not come at the cost of mothers lives.
Still don’t quite believe me?
Lets look at Victoria. As any Melbournian would tell you they had the strictest, longest lockdown in the world.
AIHW data tell us that they had the largest uptake of telehealth (by telephone) in Australia. 15% of their reduced visits were by telephone.
The AIHW figure below shows Victoria had far and away the worse stillbirth rate in Australia in 2020 rising from 6 per thousand in 2017-2019 to 8.7 per thousand in 2020.
I hope you have grasped my point by now.
When planning a response to wide-scale heath events in the future, the impact of reducing or disrupting antenatal service provision should be balanced against risks of such a strategies.
AND
If there are remnants of antenatal service provision enacted in 2020 remaining in the current Australian maternity system , such as the use of telephone visits. Can we PLEASE discontinue these services and return to safer management of antenatal services that existed prior to March 2020 as a matter of urgency?!!
FINALLY I hope that the promised inquiry into Australia’s handling of the Pandemic will include a detailed examination of the impact of changes in antenatal care provision so that we NEVER AGAIN adopt any kind of care in pregnancy that is not solidly based in evidence even if we think we might have good reason.
In memory of the 100
- New antenatal care provision recommending shorter visits, less often , was quickly enacted in Australia based on fear of Covid-19 infection in pregnancy. We knew at the time of making this change that poor antenatal visit attendance is strongly associated with poor pregnancy outcomes such as stillbirth. Whoever made this decision, took a gamble that the COVID-19 infection might have higher morbidity and mortality than the well known negative impact of reduced antenatal visits on pregnancy outcome. Turns out they were wrong.
When planning a response to wide-scale heath events in the future, the impact of reducing or disrupting antenatal service provision should be balanced against risks of such a strategies.
AND
If there are remnants of antenatal service provision enacted in 2020 remaining in the current Australian maternity system , such as the use of telephone visits. Can we PLEASE discontinue these services and return to safer management of antenatal services that existed prior to March 2020 as a matter of urgency?!!
FINALLY I hope that the promised inquiry into Australia’s handling of the Pandemic will include a detailed examination of the impact of changes in antenatal care provision so that we NEVER AGAIN adopt any kind of care in pregnancy that is not solidly based in evidence even if we think we might have good reason.
In memory of the 100
 RSS Feed
RSS Feed
